The Royal Pharmaceutical Society Becoming the Royal College of Pharmacy: What Would it Mean for Pharmacists?
- The Royal Pharmaceutical Society is required to promote the interests of pharmacists. The Royal College of Pharmacy would be required by law to act for the public benefit. The loss of representation of pharmacists’ interests is significant.
- Pharmacists would no longer have a professional (representative) body if the change goes ahead.
- If the definition of a profession set out previously in Dale and Appelbe’s Pharmacy Law and Ethics is correct, “pharmacist” would cease to be a profession.
- Pharmacists would lose control over material aspects of the way the organization is run. For example, the organization's most senior board, the Board of Trustees, would determine the regulations which make up its own constitution. It could be comprised partly or wholly of non-pharmacists, and RPS members would not be able to prevent this. The same applies to the “Senate” – the proposed replacement for the RPS Assembly. The Board of Trustees could decide that the Senate, including the role of President, would be comprised of unelected non-pharmacists.
- The most senior board – the Board of Trustees – would be able to introduce associate membership categories, for example of pharmacy technicians and dispensing assistants. Pharmacists would have no power to prevent this.
- The RPS’s assets, accrued by members from contributions made since 1841 and used for their benefit, would effectively be appropriated, gifted to charity and repurposed for the public benefit.
- Set against the disadvantages, the potential advantages of the RPS becoming a royal college are, at best, limited.
In Whose Interests Would the Royal College Act?
A good starting point is to examine the RPS’s current royal
charter, which sets out and governs how the RPS must operate as an
organization. The RPS’s entire approach and ethos is determined by the objects defined
in the charter.
The first object listed in the charter is: “(1) to
safeguard, maintain the honour, and promote the interests of pharmacists
in their exercise of the profession of pharmacy” (Emphasis added).[1]

This primary object clearly requires the RPS to act in the
interests of pharmacists.
If the RPS becomes a charity and a new royal charter is
adopted, that obligation will cease to exist. One of the legal requirements for
charity status, set out in the Charities Act 2011, is that the organization
must operate for the public benefit[2]
(see ss.1(1)(a) and 2(1)). If the organization becomes both a royal college
and a charity, this overriding requirement will dictate how the organization
operates.


In practical terms, this means that the RPS – an
organization that acts in the interests of pharmacists – will be replaced by
one that acts in the interests of the public. There are already many such
organizations. For example:
- The Department of Health and Social Care has a duty
to act in the public's interest.
- The General Pharmaceutical Council, as a regulator,
must prioritize public interests.
- The NHS is mandated to operate for the public's
benefit.
- Numerous public and consumer groups also advocate
for the public.
In contrast, there are few organizations solely dedicated to advocating for pharmacists, and only one which functions as the professional body (the RPS).
The RPS first
published the draft version of the proposed new charter on 12 February 2025. It
can be seen in the tracked changes version that the current primary object, which
requires the organization to promote the interests of pharmacists, has been
deleted.[3]

The draft proposed charter makes clear that the royal
college would be yet another body promoting compliance (alongside
employers, the GPhC, the NHS, the MHRA and others.) It would transition from
being a body which serves the interests of its members to an organization which
expected those members to comply with its diktat. Article 4 of the proposed
charter provides that the college’s powers would include:
“(2) to promote compliance with good practice and
the law, and to establish and promote professional standards amongst healthcare
professionals engaged in the practice of pharmacy;”. (Emphasis added).
![]()
The charter does not define what is meant by “healthcare
professionals engaged in the practice of pharmacy.” If the Board of
Trustees were to interpret this as including pharmacy technicians (whether or
not this is correct is a separate issue), it would then be setting standards
for them as well. Over time, some would be likely to argue that this should
entitle pharmacy technicians to membership.
No Longer a Professional Body?
I use the term “professional body” as shorthand for
“professional representative body”—an organization that represents the
interests of the profession and provides a voice for it.
The Royal Pharmaceutical Society of Great Britain (now
operating under the name Royal Pharmaceutical Society) has long been recognized
as the professional body for pharmacists, providing them with a voice. While some
may take the view that it fails in this role on occasion, that may well reflect
a problem with its leadership rather than its charter—the document that governs
its obligations. It does not reflect a problem with the provision in the RPS’s
charter which requires it to promote the interests of pharmacists.
There are other organizations that act—or at least are meant
to act—in the interests of pharmacists. If the RPS were to become a royal
college, there would be nothing to prevent another body from taking the RPS’s
place as the professional body. However, this is not part of the RPS’s
proposal, nor is it suggested in any other proposal, and nor has it been
discussed by the profession. The RPS has not identified any organization that
would take on the role of representing pharmacists’ interests if it transitions
to a royal college.
A royal college may instead label itself a “professional
leadership body” or similar, implying that it acts professionally and holds a
leadership role, and indicating that it is an organization. However, this
terminology introduces a subtle but significant shift in meaning. There is a
material difference between a “professional body” (as defined above) and a “professional
leadership body.” A professional body represents the profession, whereas a
professional leadership body could lead anything while acting
professionally. Almost any pharmacy organization could call itself a
“professional leadership body.”
Since the term “professional body” can be interpreted in
different ways (I have defined it above for the purposes of this article), some
may even argue that a Royal College of Pharmacy would still be a “professional
body”, without clarifying what they mean by the term. They might claim that the
label is appropriate simply because the royal college would be a “body”
expected to act “professionally.” However, I would suggest that generally
pharmacists are familiar with the term being used in relation to the RPS, an
organization which represents their interests. This presents a risk: the term
could be used misleadingly in relation to the royal college to suggest that it would
continue to operate in the interests of pharmacists, or that the RPS’s
representative functions would remain unchanged.
No Longer a Profession?
In Dale and Appelbe,
at the time it was edited by J.R. Dale and later Joy Wingfield and Gordon Appelbe, a section
outlined the four essential requirements for status as a profession. One of
these requirements was having a “representative body of practitioners,” and the
Royal Pharmaceutical Society of Great Britain (RPSGB) was specifically
identified as fulfilling that role. Under the heading “The Profession of
Pharmacy,” it stated:
“If the characteristics described are accepted as the
elements of a profession, then pharmacy meets the essential requirements, which
are four in number as follows
…
2. A Representative Body of Practitioners: “The
representative body of the profession is the Royal Pharmaceutical Society of
Great Britain. The Council of the Society is elected by the members and its
functions include control over educational standards for pharmaceutical
chemists. It also guides the profession in establishing and interpreting a code
of conduct.”
If we no longer have a representative body of practitioners,
then according to Dale and Appelbe,
we would no longer meet the criteria to be considered a profession. Notably,
this section has been removed in the most recent edition, after being included in Dale
and Appelbe for at least 42
years, from at least 1979 to 2021.
The requirements for professional status in Dale and
Appelbe were set out at a time when the RPSGB served both as the regulator
and the professional body. In 2010, these functions were separated: the General
Pharmaceutical Council (GPhC) became the regulator, and the Royal
Pharmaceutical Society (RPS) became the professional body. It is difficult to
see how this changes the underlying requirement for a representative body of
practitioners, even if the representative functions of the body now reside
only with the RPS.
The examples given in Dale and Appelbe of the
functions of the “representative body of practitioners” concern the ability of
pharmacists to exert control over their own leadership within that body, and
through that control, to determine their own future, standards and education,
and to better the profession. Today, the RPS is the body which most closely
fits that description. Members elect its boards to serve their interests, and
the Assembly is appointed from within the boards; the boards and Assembly govern
the organization; and the RPS has the ability to encourage higher standards
including in respect of education. It does not have the ability to control
minimum standards or educational requirements required for registration as a
pharmacist; those functions rest with the GPhC, and are not controlled by the
profession. Only through the RPS, and not the GPhC, can the profession exert a
significant degree of control over its own future.
If the RPS transitions into a Royal College of Pharmacy, the following
consequences would arise in relation to the organization:
- It would no longer be under pharmacists’ collective control. Pharmacists, among others, may have a say, but they would not have authority over the organization insofar as, for example, they could not remove members of the most senior board – the Board of Trustees.
- It would not have an object requiring it to
represent pharmacists’ interests.
- Its governing board at the highest level in the
organization would not be elected by pharmacists.
- There would be no requirement for the Board of
Trustees to include pharmacists among its members.
- It would not control the standards of initial
education and training. This responsibility was transferred to the GPhC in
2010 and depends on government decisions. Credentialing, which the RPS can
already undertake, would still rely on recognition by employers, including
government-linked organizations like the NHS.
- Its membership numbers—if similar to those of the
RPS—would likely represent less than half of the profession.
- It would act in the interests of the public, which
may conflict with the interests of pharmacists.
In effect, there would no longer be a “representative body
of practitioners” in any meaningful sense of the term.
Later editions of Dale and Appelbe incorrectly
identified the GPhC as the “representative body of practitioners”. This was a
misinterpretation of the original text. Individuals do not become members
of the GPhC; they merely register with it, because they are statutorily
required to do so if they wish to call themselves pharmacists. The GPhC does
not represent their interests. It is not a body of practitioners through which
pharmacists can express any shared goal or purpose. Practitioners exert no
control over it and do not join it out of care or any sense of belonging, unity
or collective desire for betterment. Registration is imposed upon them. The
requirement for a “representative body of practitioners” is not satisfied
merely by having an organization registering a large number of pharmacists. For
similar reasons to those set out above illustrating the reasons that a royal
college would not be a representative body of practitioners, nor would the
GPhC.
The Core Question: Would Pharmacy Still be a Profession?
Dale and Appelbe raised a compelling point: if a group
of practitioners cannot maintain the existence of its own representative body, can
it still legitimately call itself a profession?
Claimed Advantages of Becoming a College
The current leadership of the RPS is asking you to vote in
favour of becoming the Royal College of Pharmacy. This is questionable in
itself: how can the RPS leadership be said to be promoting the interests of
pharmacists in proposing to convert the organization into one which acts in
the interests of the public instead?
The RPS leadership suggests that there are certain
advantages to the proposed transition, such credentialing and having a louder
and more effective voice for pharmacy – not pharmacists.[4],[5]
However, these are activities it could already undertake as the Royal Pharmaceutical Society. It already performs credentialing, which involves designating individuals as having reached a particular level of performance in their careers. If it seeks a louder voice, what does that entail? What prevents it from achieving that now? It already has the ability to decide its approach to engaging with other organizations and the press, and the topics it addresses. Perhaps more importantly, the college would not be providing a voice for pharmacists or pharmacy at all: it would have no objects to do so, would act for the public benefit, and to provide such a voice may conflict with this and its duties as a charity.
My view is that the advocates of becoming a royal college
are not suggesting the organization will suddenly gain new capabilities. The
point they are making is more subtle, and they have not clearly articulated it.
If the RPS becomes a royal college and a charity, it will
have a legal duty to act for the public benefit, rather than in the interests
of pharmacists as at present. This change could make the organization’s
recommendations more palatable to the government. Currently, since the RPS has
a duty to promote the interests of the profession, it could be seen to be
credentialing pharmacists to enhance their standing. However, if its duty
shifts to acting for public benefit, the credentialing it carries out may hold
more inherent value to the civil service. It is worth noting that the civil
service itself initiated this proposed transition by establishing a “Pharmacy
Professional Leadership Advisory Body”. A duty to act for the public benefit
would be consistent with the functions of the civil service.
The reason the current RPS leadership has not explained this
fully may be that doing so would involve explicitly drawing attention to the
fact that the college would be acting in the public interest rather than in the
interests of pharmacists. The implications of this significant shift have not
been clearly communicated. The lack of transparency from the RPS is a recurring
issue; for example, when the RPS announced its proposal to become a royal
college, it stated that this was partly based on an independent report
highlighting its transparency problems.[6]
Other RPS PR material related to the proposed change claims
that “the pharmacy landscape is changing rapidly” and that the
organization needs to be “stronger” (without defining what this means or
explaining how the proposed changes would achieve it) and “more flexible”
(without specifying in what way, how becoming a royal college would achieve
that, or explaining why this is necessary).[7]
These arguments are weak and are worth
noting only because they are vague and lack substance.
Finally, some may argue that a royal college would be more
“collaborative” or “inclusive” than the RPS. These terms may be used in place
of substantive arguments for change or as a means of exerting control or
suppressing dissent. Such rhetoric could discourage opposition, as critics may
fear being labelled as “not inclusive”—a term that can imply an unwillingness
to work with others. However, the RPS already has the ability to collaborate
with others. Moreover, a body representing the interests of a single profession
must, in certain respects, maintain a degree of exclusivity / non-inclusivity to
effectively fulfil its representative functions.

Limited Benefits of Royal College Credentialing
In pharmacy, several factors limit the benefits of credentialing or other
functions a royal college might perform. Control over initial education and
training, entry into the profession, accreditation of courses, and the ability
to include annotations on the register for those with postgraduate
qualifications or credentials has already been ceded by statute to the GPhC.
This constrains any role a royal college might have in setting standards.
Under the current system, there is nothing to prevent the
GPhC from considering RPS accreditations and granting register annotations for
those who achieve them. This would involve the profession establishing a
standard and determining who meets it, but GPhC approval would still be
required—just as it is now for Independent Prescribers. The GPhC’s role ensures
public protection by validating any steps taken by the RPS. If such public
protection already exists, it obviates any need for a credentialing body to be
acting for the public benefit. Consider the position of universities awarding
the MPharm degree: they are not required to act solely for the public benefit.
The GPhC provides the quality assurance in respect of University graduates.
Another limitation is that employers must value
credentialing for it to be impactful. The skills and expertise denoted by
credentials would need to align with employer needs, which might not always
align with pharmacists’ career aspirations. For example, in community pharmacy,
for businesses focused on minimizing costs, credentialing may hold little
relevance. The business model might prioritize hiring pharmacists as
inexpensively as possible, regardless of credentials. Thus, the RPS becoming a
royal college is unlikely to increase demand for credentialing among such
employers.
Modern Charters
An updated charter would likely require the RPS to operate for the public benefit, as this is a fundamental requirement of modern charters. There is no inherent positive connotation to the term “modern” here, as is sometimes implied. Modernization is only beneficial if the changes themselves are positive. It is damaging if the changes are damaging.
Organizations receiving charters today are expected to work
in the public interest. The Privy Council’s website explains:
“Their original purpose was to create public or private
corporations (including towns and cities), and to define their privileges and
purpose. Nowadays, though Charters are still occasionally granted to cities,
new Charters are normally reserved for bodies that work in the public interest.”[8]

While the RPS would not receive an entirely new charter, it would
be asking the Privy Council to materially update it, potentially mandating the
RPS to operate for the public benefit. This requirement would align with its
potential status as a charity, since a charity must act for the public
benefit. A charter that conflicted with this mandate by prioritizing other
objectives would be incompatible with charitable status.
Even if the RPS ultimately decided against becoming a
charity, a royal college might still be expected to serve the public interest
if the charter were materially updated.
Ability for Pharmacists to Control the Organization
Another important consideration is the governance structure of the proposed royal college. If the RPS becomes a royal college, pharmacist members would no longer have the authority to remove members of the most senior governing board. As a charity, this would be the Board of Trustees. Currently, RPS pharmacist members can vote for board members and replace them after three years if desired. This provides a mechanism to remove many of the members of the RPS Assembly, who are appointed from among the members of the board. The royal college would still have an assembly – renamed to the Senate – but its powers would effectively be passed to the Board of Trustees. The Board of Trustees could also decide the constitution of the Senate – so it could decide, for example, that the members of the Senate, including the President, would not be elected, or that it would be comprised entirely of non-pharmacists.

The governing board could make significant changes, such as introducing new associate membership categories, for example of pharmacy technicians. Historically, the inclusion of pharmacy technicians has been a long-term goal of some individuals pushing for the RPS to become a royal college. Some of the same individuals were proponents of the inclusion of pharmaceutical scientists in associate membership.
The number of pharmaceutical scientists who are associate
members of the RPS is low. I was once told the figure – it was of the order of
around 10 to 20, among tens of thousands of pharmacist members. Despite this,
the RPS often emphasizes “pharmaceutical scientists” in its communications,
reflecting their inclusion in its remit. More broadly, the RPS frequently
refers to its role as supporting "pharmacy" rather than
"pharmacists," as seen in its mission statement: “Our mission is to
put pharmacy at the forefront of healthcare.”[9]
On social media, immediately below its name, it states: “We are the
professional leadership body for pharmacists and pharmaceutical scientists.”
It has no duty to represent the interests of pharmaceutical scientists, but it
is clear that their associate membership influences its behaviour nonetheless.

Examination of Other RPS Charter Objects
Before considering a shift to royal college status, it is
worth further examining the RPS’s current objects.[10]
- to safeguard, maintain the honour, and promote
the interests of pharmacists in their exercise of the profession of
pharmacy.
- This object explicitly focuses on
benefiting pharmacists and upholding their professional interests.
- to advance knowledge of, and education in,
pharmacy and its application, thereby fostering good science and practice.
- This object benefits the profession
through the advancement of pharmacy knowledge, with an indirect impact on
the public.
- to promote and protect the health and well-being
of the public through the professional leadership and development of the
pharmacy profession.
- Here, public well-being is a
secondary outcome achieved through professional leadership and
development. The primary focus remains the professional interest.
- to maintain and develop the science and practice
of pharmacy in its contribution to the health and well-being of the public.
- This object acknowledges the public
benefit of developing pharmacy science and practice but keeps the
profession central to its mission.

Each of these objects prioritizes the profession and its
members, with public benefit as an associated outcome. This is fundamentally
different from the proposed royal college objects, which would directly
prioritize the public benefit.
RPS Assets
Consider the implications for the RPS’s assets under its existing charter:
“4. The income
and property of the Society shall be applied solely towards the promotion of
the objects.”

If the RPS becomes a royal college, the assets it has
accrued over many years—through the contributions of pharmacists—would no
longer be put to use for their direct benefit. Instead, these assets would be
given over to the royal college as a charity, and redirected toward serving the
public. While they would still support the organization’s stated objects, those
objects would have shifted to prioritize public benefit rather than the
interests of pharmacists.
The Name of the Organization
The proposed name for the new royal college—The Royal College of Pharmacy, not The Royal College of Pharmacists—offers
a significant clue about the intentions of those advocating for this change.
Consider the naming conventions of other royal colleges associated with
healthcare professions. With two exceptions—the Royal College of Nursing (RCN), which has an older charter requiring it to act in the interests of nursing and midwifery professions, and the Royal College of Emergency Medicine,
which serves Emergency Physicians—these organizations are typically named after
their professions. Examples include the Royal College of Physicians, the Royal College of
General Practitioners, the Royal College of Radiologists, and others.[11]

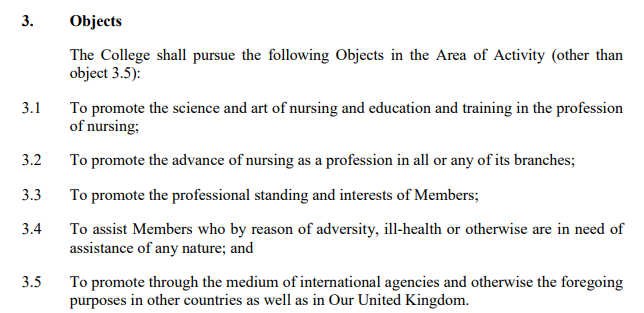
The objects of the RCN charter are shown below.
“Pharmacy” is a scientific field. It is also an area of
study, a field of practice, and a type of business. It is not the noun that
specifically refers to the profession as a group of people—pharmacists. The proposed name, therefore, raises the possibility
that the new royal college may be subject to influence from various external
entities, such as pharmacy businesses, universities, the pharmaceutical
industry, and wholesalers. A royal college would act “for the public benefit”,
and to varying degrees, each of these types of organization serves the public
interest. The voice of pharmacists within the college could be very much drowned out among these
competing voices.
You can be confident that the Royal College of
Pharmacy will not limit its membership to pharmacists for very long. While
proponents may claim that there are no immediate plans as part of this change to
expand membership beyond pharmacists, history suggests that this would change
soon after the ink is dry. Pharmaceutical scientists have already been given
associate membership, and it is only a matter of time before pharmacy
technicians and potentially other groups are added.
It is clear from the proposed charter that pharmacists would
be unable to prevent the Board of Trustees from adding new associate membership
groups. It provides, under article 7:
“(2) The Board of Trustees may establish one or more
categories of associate membership, but such Associate Members are not Members
of the College for the purposes of this Our Supplemental Charter.”
(3) Subject to this Our Supplemental Charter, Members and Associate Members of the College shall have such rights, privileges and obligations (and may be charged such subscriptions) as may be specified in Regulations.
If an organization represented both pharmacists and pharmacy
technicians, it would create an irreconcilable conflict of interests. These
groups compete over costs, roles, and responsibilities. Pharmacy technicians
have recently been authorized to deliver PGDs (Patient Group Directions), and a
substantial consultation in 2024 proposed allowing them to supervise the sale
and supply of medicines.
However, an organization serving the public interest would represent neither of these groups. If the royal college prioritized the public interest, its decisions may well align with the preferences of the civil service. Should the civil service determine that pharmacy technicians should take on additional roles, the royal college may comply, producing compliant corresponding policy. Similarly, if it decided that pharmacists should perform specific tasks, the royal college may be keen to follow suit.
Member Duties to the Charity
Members may potentially have a duty to act in the best interests of the charity, for example when exercising their voting powers. The Charity Commission has taken this view for many years - see RS7 - Membership Charities at pages 18 and 34 (https://www.gov.uk/government/publications/membership-charities-rs7). In turn, the charity acts for the public benefit. Some may argue that members would have a duty to vote in a way which increase the charity's revenue, for example by introducing new members.
The juxtaposition of the current position with the proposed one is striking: currently the RPS has an object to promote the interests of pharmacists. As a college, members may find themselves with a duty to act in the best interests of the organization.
In Everyone Else’s Interests but Pharmacists’?
If pharmacists lose an organization that advocates for their
interests, who will oppose policies that work against them? If other
stakeholders decide to impose unfavourable conditions on pharmacists, they will
face less resistance if the RPS cannot even theoretically stand in their way.
Contractors as contractors, for instance, are unlikely to oppose the
transition. They may even support it, recognizing that a royal college focused
on the public benefit may be less likely to challenge the conditions imposed on
pharmacists than an organization which is meant to act in pharmacists’
interests.
Similarly, the civil service has no incentive to oppose the
change. At present, the RPS is a body that can challenge civil service
proposals. For example, under Martin Astbury's presidency, the RPS resisted
certain pharmacy supervision proposals from the Department of Health and Social
Care (DHSC). If the RPS becomes a royal college, this capacity for resistance
diminishes, making it easier for the civil service to implement its policies
without opposition.
Unions and indemnity insurance providers may also be
unlikely to object. Historically, there has existed the possibility that the
RPS would become a union or an indemnity insurance provider, creating
competition in the sector. However, a royal college acting for the public
benefit, particularly if it also becomes a charity, would not do so. The risk
of competition would fall away if the transition to a royal college went ahead.
Whose Interests Should the RPS Serve?
Some might argue that acting for public benefit aligns with their
own motivations as a pharmacist. After all, pharmacists work to serve the
public. However, that does not mean the professional body should prioritize the
public interest over pharmacists’ professional interests. The role of a
professional body is to represent and advocate for its members.
Some might think, "But I’m a member of the public
too!" While this is true, in their capacity as a pharmacist, they require
a professional body to act specifically in their interests. Many organizations
already work to serve the public. A counterbalance is necessary: a body that
speaks solely for the profession. Currently, the RPS serves this role.
If the RPS transitions to a royal college, this critical
balance is lost. It will no longer act as a voice for pharmacists, leaving pharmacists
without the organization’s much-needed representation.
In What Ways Could the Professional and Public Interest Conflict?
Consider the situations in which the interests of the public
might conflict with those of pharmacists. The Assisted Dying Bill provides a clear illustrative example. From the
public's perspective, Parliament might deem it beneficial for assisted dying to
be available, provided adequate protections are in place. Public sentiment
might support requiring pharmacists to sell or supply the necessary drugs.
Alternatively, the public might expect pharmacists to refer patients to someone
else who can provide these drugs, even if the pharmacists themselves object on
ethical grounds.
Pharmacists, however, might object to participating in
assisted dying, whether directly or indirectly. Their objections could stem
from ethical, religious, or societal concerns, such as a belief that palliative
care should be prioritized and improved rather than offering assisted dying as
an option. These objections could place pharmacists in an ethically fraught
position if they are required to supply the drugs or refer patients to others
who will.
The RPS took a position saying that pharmacists should be
able to exercise conscience, and should not be put under any duty to refer to
someone else would provide the service.[12]
It said:
“Conscience clause - It is a
pre-requisite that a conscience clause is incorporated into any legislation.
There must be no obligation for any pharmacist to participate in any aspect of
an assisted dying or similar procedure if he or she feels this is against their
personal beliefs. The framework we are proposing allows pharmacists to ‘opt in’
by completing the necessary training, rather than ‘opting out’. It also avoids
the need for anyone ethically opposed to assisted dying to signpost to another
pharmacist as this can also pose an ethical dilemma.”
However, if the RPS were to become a royal college with a
duty to act for the public benefit, it might adopt a different stance. For
example, it could advocate for a duty requiring pharmacists to provide the
service or at least to refer patients onward, creating a conflict between
pharmacists' professional autonomy and the perceived needs of the public. The
college’s proposed objects include relieving sickness.[13]
The Board of Trustees, which may be comprised partly or entirely of
non-pharmacists and in any event would be required to fulfil the role set out
in the object, may consider that this requires them to adopt a different
position on assisted dying to that advanced by the RPS.
![]()
Another example of potential conflict is the matter of
professional remuneration. Pharmacists may seek higher fees for their services,
while the public—and by extension, government policymakers—may favour
delivering those services as cheaply as possible. This could lead to tasks
being delegated to pharmacy technicians or other less-qualified personnel to
reduce costs. A royal college acting in the public interest might support these
cost-saving measures, even if they are detrimental to pharmacists’ professional
and financial interests. Such actions would align with the interests of
businesses and the civil service, but not necessarily those of pharmacists.
A Royal College As Well?
Having a royal college could offer benefits to the public,
such as credentialing potentially having a higher value, and standard-setting
within the profession. However, an increased focus on credentialing could also
have drawbacks. If employers began requiring specific credentials from
pharmacists, membership of the royal college might become mandatory, or
effectively mandatory. This would increase costs for pharmacists, as they would
need to pay membership fees to the college in addition to their registration
fees with the GPhC. Despite this financial burden, wages might not
increase to offset the additional costs. It would benefit the public to have
better services at lower cost.
Furthermore, if the RPS becomes a royal college, its
financial stability might depend on its ability to compel pharmacists to obtain
credentials through the college. The college could charge for credentialing
directly, or increase general membership fees. To ensure a steady revenue
stream, the college would have an interest in encouraging employers to require
these credentials, forcing pharmacists to join and pay for membership and/or assessments.
While there are potential benefits to having a royal college
in terms of advancing professional standards, forming such an institution by
transforming the RPS raises significant concerns. If the RPS becomes a
royal college, pharmacists would lose their current professional representative
body. Surprisingly, the RPS has not addressed this issue in its proposals,
leaving a critical gap in the discussion.
The RPS does not appear to have set out to inform pharmacists of
the risks and adverse consequences of the proposed transition. Instead, it has
chosen to campaign solely in favour of the proposed change.
It is worth considering whether a Royal College of Pharmacists or a similar institution could be
created separately, leaving the RPS intact to continue representing
pharmacists’ professional interests. However, simply transitioning the RPS into
a royal college—particularly a college of pharmacy, which may prioritize
the broader field over the profession—risks leaving pharmacists without
effective representation.
What Should be Done?
A consideration with having a royal college in pharmacy is
that we already have a royal body, the Royal Pharmaceutical Society, and it is
our professional representative body. Would it be problematic to have both the
Royal Pharmaceutical Society and a Royal College of Pharmacists?
Rather than rushing to support the RPS’s transition into a
royal college, it’s vital to consider the broader implications. If a royal
college was to be established from the RPS, the profession should consider whether
it could simultaneously create a new representative body for pharmacists.
Without this, pharmacists would be losing a voice in critical areas such as
wages, working conditions, and professional autonomy.
The creation of a new representative body for pharmacists
would require careful consideration. The RPS has a charter conferred by the monarch,
facilitated by the privy council. To that extent, its operations and governance
have been subject to scrutiny and approval, which to an extent adds gravitas to
its activities and provides a degree of assurance. It occupies a unique
position at present, in that the civil service often includes it in discussions
about policy change affecting the profession. If it did not, it would not be
seen to have consulted the profession.
It would not be possible to create another organization with
the same position and status as the RPS, once the RPS ceased to exist in its
current form. A modern royal charter would not allow such an organization to
operate in the same way, and in any event there has been no suggestion of
creating a second organization with a royal charter. If one was going to
recreate the RPS, then why change the RPS to a royal college in the first place?
Relative to the role of the RPS, the roles of other existing
organizations in pharmacy are limited in scope (for example, to defence rather
than active representation), and the civil service often appears not to want to
listen to them. It does not include them in key policy discussions. It may say
that it has no reason to, where it is engaging with the RPS, because it is
already listening to the profession. In future, it is possible that it would
seek to engage only with a royal college, pretending that this is the mechanism
by which pharmacists’ views are represented, but leaving pharmacists with no
representation of their interests to government.
The civil service has to act in the public interest; it is
not its role to identify or ensure professional representation for pharmacists.
There is little wonder that it has demonstrated little if any care, in the
process which has led to the present proposal, for whether pharmacists retain
representation of their own interests. That is not its concern.
A thoughtful and transparent discussion is needed. Proposals
for a Royal College of Pharmacists or similar institution could be
discussed alongside plans for maintaining a professional representative body.
This approach would ensure that pharmacists would not lose their representation
or find themselves paying higher fees without corresponding benefits.
Until these issues are addressed, in my view it will be prudent
to vote against the current proposals to transform the RPS into a royal
college. Doing so will better protect pharmacists’ professional interests and help
to ensure that the conversation moves in a direction that benefits the
profession as a whole.
Whose Interests Should a Professional Body Represent?
There is research and other discourse which has considered the question of
whose interests should be represented by a professional body. Some of this
dates back to times where it was common for the same organization to function
as the regulator and the professional body (see for example a paper by Harvey
and Mason in 1995[14]).
That used to be the case with the RPSGB before it was renamed to the RPS and
became solely the professional body, and a separate regulator – the General Pharmaceutical
Council – was created. The
RPSGB was both the regulator meant to act in the interests of the public, and
the professional body meant to act in the interests of the profession. There
was an obvious conflict. It was for this reason that the RPSGB’s functions were
split. The RPS’s present proposal is that both bodies created by the split will
ultimately serve the public – some may view this as an unfair outcome
for pharmacists!
Some of the discourse which examines whether a professional
body should represent the interests of the public or those of the profession reaches
conflicting conclusions. Some older research papers are likely to have been
affected by the fact that they've had to consider professional bodies working
with a dual role. Further, in reaching conclusions, where consideration has
been given to the extent to which the professional body should serve the
interests of the public, it is recognised that such service by a professional
body would be indirect, ultimately with the intention or objective of serving the
interests of the profession.
It has been posited that in serving the public, the
profession will ultimately serve its own interests because it will be seen to
be acting with selflessness and altruism, which will increase the prestige and
trustworthiness of the profession. This perspective, however, seems a flawed way
to look at the function of a professional body. The profession should
act with selflessness and altruism in its work, and it has a regulator which
requires it to do so. The professional body will be aware of this. But through
its professional body, it should have an organization looking after its
interests directly. Further, the aforementioned posited contention is naïve, in
that it does not take into account the potential for interference from those
with vested interests, and corporate capture (where businesses use their
political influence to take control of the decision-making apparatus of an
organization).
In considering the question “in whose interests should the
professional body act directly?”, it would not make sense for the answer to be “the
public’s” and the benefit to the profession being sometimes a side effect, if
the ultimate intention is to serve the professional interest. In such a case,
where the interests of the public and the profession conflict, it would always be
the interests of the public which would win out. The profession would have to
take a back seat – its interests would be secondary. It might be the case that
in acting in the interests of the profession, a professional body would offer some
consequential benefit to the public because, for example, in increasing the
standards of education and training, whether that be initial or postgraduate
education and training, that would result in a higher overall level of skill
and competence from which the public would benefit. It should be viewed from
that perspective rather than the opposing one. Which other organization is
going to act in the interests of the profession, if not the professional
body?
One limitation of the research I’ve encountered is its
narrow focus on specific functions of professional bodies, such as raising
educational standards. While educational standards are undeniably important,
other crucial functions often receive limited attention. These may include:
- The provision of professional indemnity insurance
- The services of a trade union
- Offering professional advice
- Responding to political developments
- Interfacing with the media
- Liaising with policymakers and MPs
- Raising the profession’s profile
A professional body acting solely in the public interest
would struggle to perform many of these functions effectively, as they may not
align directly with the public interest or might even conflict with it. For
instance, advocating for better pay or working conditions for pharmacists may
not always be seen as benefiting the public, but it is critical for the
profession’s well-being.
There is also the question of whether the conflict of
interest between being a regulator and a professional body is so significant that
it warrants their separation, balanced against the benefits of having
professional expertise within the regulator. While this debate is valid,
Parliament has already determined that the two functions should remain
separate. For the civil service to suggest that both the regulator and the organization
which is currently the professional body should act solely in the public
interest goes a step too far. If both bodies serve the public, what remains to
protect and promote the profession’s interests?
How Should the RPS have Reacted to the UK Pharmacy Professional Leadership Advisory Board?
The Royal Pharmaceutical Society (RPS) holds a relatively
strong position within the profession. In my view it should have maintained
independence from the UK Pharmacy Professional Leadership Advisory Board (UKPPLAB),
responding to its recommendations with an acknowledgment that professional
leadership must ultimately be decided by the profession, not the civil service
or its appointees. By participating in UKPPLAB, the RPS positioned itself as
subordinate to the board and lent its credibility to the UKPPLAB – though it
was perhaps influenced by a desire to preserve its own standing and avoid embarrassment.
This is of no disrespect the civil service. When it comes to
professional leadership, the RPS is the existing body representing the
profession—not an entity created by the civil service. Some may view the Chief
Pharmaceutical Officers (CPhOs) who established UKPPLAB as senior figures whose
input must be heeded. Within the civil service hierarchy, this may be true.
However, as members of the pharmacy profession, their opinions are no more or
less valid or important than those of any other pharmacist. Professional
leadership should not be determined by civil service appointees, but by the
profession itself.
The RPS should in my view have asserted its independence by
declining to participate in UKPPLAB meetings, instead stating, for example: “We
appreciate your recommendations, but the leadership of the profession must be
determined by the profession, not the civil service or its representatives.”
Had the RPS taken this stance, the UKPPLAB’s recommendations
would have carried the appropriate weight. They’d have been recommendations,
and no more. Instead, by joining the board, the RPS allowed itself to be
influenced, potentially compromising its role as the profession’s advocate.
Could the Royal College Receive Charitable Donations From Pharmacy Contractors, Wholesalers and Pharmaceutical Manufacturers, for example?
Yes.
An example of this can be seen in the case of the Royal
College of General Practitioners, here: https://www.telegraph.co.uk/news/2025/01/11/royal-college-of-gps-conflict-childrens-covid-jabs
Two quotes from the article:
·
“However, Prof Marshall failed to declare
that the Royal College had previously received payments from Pfizer, the only
pharmaceutical company at the time with a Covid vaccine authorised for use in
children.
Prof Martin Marshall
Prof Martin Marshall, who was chair of the
Royal College of GPs at the time of the pandemic and spoke at a key meeting
During 2021, it received more than £100,000 from
Pfizer, according to the Association of the British Pharmaceutical Industry
(ABPI).
Their register shows that during that calendar
year, £102,820 was given for “donations and grants” as well as “benefits in
kind”.
This was more than double what the organization
received the previous year from Pfizer –
£49,324 – and up from £4,309 in 2019 for event sponsorship, donations, grants
and benefits in kind.”
·
“A spokesman for the Royal College of GPs,
said: ... “The College’s income from Pfizer for the year ending March 31 2022
was related to educational resources on migraine and arthritis, amounting to
0.26 per cent of total RCGP income, and had no bearing on discussions related
to the pandemic.””
Could such donations influence the behaviour of the
organization? A more incisive question might be: What Board of Trustees is likely
to act in ways that could alienate or offend its major donors?
Use of Members’ Funds
One of the proposed objects of the royal college, set out in
the proposed charter, is:
“(c) to relieve poverty, financial hardship or other
distress among current and former Members and Associate Members of the College
and development of the pharmacy profession;their dependants and among those
studying or training to be a pharmacist, and such others who practice or
have practised the profession of pharmacy as the Trustees may determine from
time to time.”[15]
(Emphasis added).
Various questions arise from this object, including:
· How would the Board of Trustees define “others
who practice or have practised the profession of pharmacy”? Would they
interpret this as including pharmacy technicians and dispensing assistants
(again the accuracy of this interpretation would involve a separate debate),
and if so would this object allow the Trustees to give away the college’s
funds, including those derived from pharmacists’ membership fees, to non-pharmacists?
· What would be the implications for Pharmacist
Support – a charity which already exercises some of these functions?
Appointment of Trustees
The Board of Trustees will be appointed in accordance with
Regulations created by the Board of Trustees. The trustees may or may not be
pharmacists – there is no requirement specified in the proposed charter in this
regard.[16]
The RPS has suggested that the chair of the Board of Trustees – the chair being
the most senior position in some respects – may be a non-pharmacist, because it
requires substantial expertise in running a charity.[17]
The RPS has also expressed the “intention” that the Board of Trustees would
include a majority “drawn from the profession” – though the RPS does not say
whether it considers “profession” to be a reference solely to pharmacists, there
is nothing to provide for this within the charter, and it would be beyond the
control of the RPS. The Board of Trustees would decide this for itself. It would
be entirely within its control to decide that it should be comprised entirely
of non-pharmacists.


The “Save Our Society” Campaign
In 2003, the RPSGB proposed a new royal charter which amongst other things would have required the organization to operate in the context of the public benefit (though safeguarding, maintaining the honour and promoting the interests of pharmacists was retained). The current proposal goes further than this - the college would be entirely for the public benefit and the aforementioned object relating to pharmacists would be deleted.
The proposals in 2003 led to the “Save our Society” campaign. Four individuals brought a legal
challenge, which led the privy council to put the RPSGB Council’s proposals on ice
(see Koziol et ors. v Royal Pharmaceutical Society of Great Britain et ors.
[2004] EWHC 1254 (Ch)). As I understand it, the delay also allowed the
campaigners to field candidates who opposed the changes for election to the
RPSGB Council. Such candidates were ultimately elected, leading to the defeat of
the proposals. Against this historical backdrop, it was interesting that the
RPS cancelled its board elections for 2025.[18]
Questions Asked by the Guild of Healthcare Pharmacists
The Guild of Healthcare Pharmacists asked questions about
the proposed transition, in a letter dated 21 October 2024.[19]
These included, “In recent history Royal Colleges and the leadership of
Royal Colleges have come under intense scrutiny and criticism in medicine
during the discourse surrounding Physician Assistants/Physician Associates.
Junior/resident doctors make the point that Royal Colleges appeared to be
primarily enacting the aims of government as opposed to leading the medical
profession forward. With these fresh issues in mind, what safeguards would be
put in place to ensure that a Royal College of Pharmacy truly led for, and
on behalf of, the pharmacy profession?” (Emphasis added.) Following the
publication of the proposed charter for the royal college, it is now apparent
that the royal college would not be led for or on behalf of the
profession at all; it would be operated for the public benefit.
Special Resolution Ballot - What Majority would be Required?
(section added 20 March 2025)
The current Charter and Regulations can be found at
https://www.rpharms.com/LinkClick.aspx?fileticket=P4j2CrhkWMo%3d&portalid=0
and
https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Regulations/NEW%20REGS%20CURRENT_%20WITH%20AMENDMENTS%20RE%202025%20ELECTIONS%20-%20modified%20version%2014_02_25.pdf
respectively.
The RPSGB Assembly can make regulations (“Regulations”) pursuant to the power in Article 10 of the Charter.
Insofar as any Regulations contradict the Charter, the Charter will prevail. Insofar as they do not, the Charter gives the Regulations the same force as the Charter itself.
Article 11 of the Charter provides:
“The Society may by Special Resolution amend, add to or revoke any of the provisions of this Our Supplemental Charter or of any further Charter granted to the Society, or may amend the name of the Society, provided that any such amendment, addition or revocation or name shall not be effective unless approved by Us, Our Heirs or Successors in Council.”
Article 12 of the Charter provides, so far as is material:
""Special Resolution" means a resolution of the Assembly confirmed by a ballot of the members referred to in articles 5(1)(a) and 5 (1)(b) by not less than a two-thirds majority of the votes of such members."
The members referred to in articles 5(1)(a) and 5(1)(b) are those who are pharmacist and former pharmacist members of the RPS.
The ballot threshold in Article 12 could be interpreted as either:
i. The eligible members have votes. Two thirds of those votes must be cast in favour. As such, two thirds of all those members eligible to vote must have cast their vote in favour. (“The First Interpretation”)
ii. Of the votes cast, two thirds must be in favour. (“The Second Interpretation”)
There are good reasons as to why the First Interpretation is correct. However, even if the Second Interpretation were correct, the Regulations – at the very outset – require two thirds of eligible voters to ratify changes to the Charter.
Regulation 1.1.1 provides inter alia:
“Royal Charter
…
Any changes to the overall content of the Charter, including to the composition of the Assembly, or the creation of any additional categories of membership of the Society require a Special Resolution to be passed with the support of at least 2/3 of the Members and Fellows eligible to vote.”
If the Second Interpretation were correct, Regulation 1.1.1 would create an additional requirement, but not a contradictory one. For the vote to go ahead:
a. two thirds of those eligible to vote would have to vote in favour, and
b. two thirds of the votes cast would have to be in favour.
Both of these requirements would be satisfied if two thirds of those eligible to vote, voted in favour.
Regulation 3.4 provides, in the context of meetings (this being the heading for Regulation 3):
“‘Special Resolution’ means a resolution of the Assembly confirmed by a ballot of the members eligible to vote (ie Members and Fellows, currently in good standing) giving a two-thirds majority of the votes cast.”
Regulation 3.4 would not apply to the current ballot, because it is not being conducted in a meeting. It is otherwise in any event immaterial considering the effects of Article 12 and regulation 1.1.1. Again even if the Second Interpretation were correct, 1.1.1 would create an additional requirement irrespective of the requirements of 3.4.
Conclusion
The RPS should have presented alternative perspectives to pharmacists – that would have been acting in their interests. I hope this article helps some in making their decision on how to vote. For the reasons above, I will be voting against.
Last updated: 23 March 2025
[1]
https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Governance%20documents/text-of-the-2004-supplemental-charter-as-amended-27.09.10.pdf?ver=2016-11-08-094856-680
[2]
https://www.legislation.gov.uk/ukpga/2011/25/section/2
[3]
https://www.rpharms.com/LinkClick.aspx?fileticket=FwL02tnOxNI%3d&portalid=0
[4]
https://www.rpharms.com/about-us/changeproposals/changefaqs
[5]
https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Guidance/Roadshow%20Report_10_01_25_single%20pages.pdf
[6]
https://www.rpharms.com/about-us/changeproposals/changefaqs
[7]
https://www.rpharms.com/changeproposals/
[8]
https://privycouncil.independent.gov.uk/royal-charters/
[9]
https://www.rpharms.com/about-us
[10]
https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Governance%20documents/text-of-the-2004-supplemental-charter-as-amended-27.09.10.pdf?ver=2016-11-08-094856-680
[13]
https://www.rpharms.com/LinkClick.aspx?fileticket=FwL02tnOxNI%3d&portalid=0
[14]
http://www.qualityresearchinternational.com/Harvey%20papers/Harvey%20and%20Mason%20Professions%201995%20[2014].pdf
[15]
https://www.rpharms.com/LinkClick.aspx?fileticket=JbvxgNWBFMs%3d&portalid=0
[16]
https://www.rpharms.com/LinkClick.aspx?fileticket=JbvxgNWBFMs%3d&portalid=0
[17]
https://www.rpharms.com/LinkClick.aspx?fileticket=lJoIh8PWtGA%3d&portalid=0
[18]
https://pharmaceutical-journal.com/article/letters/raising-concerns-about-the-cancellation-of-2025-board-elections
[19]
https://www.ghp.org.uk/an-open-letter-rps-royal-college-proposal/